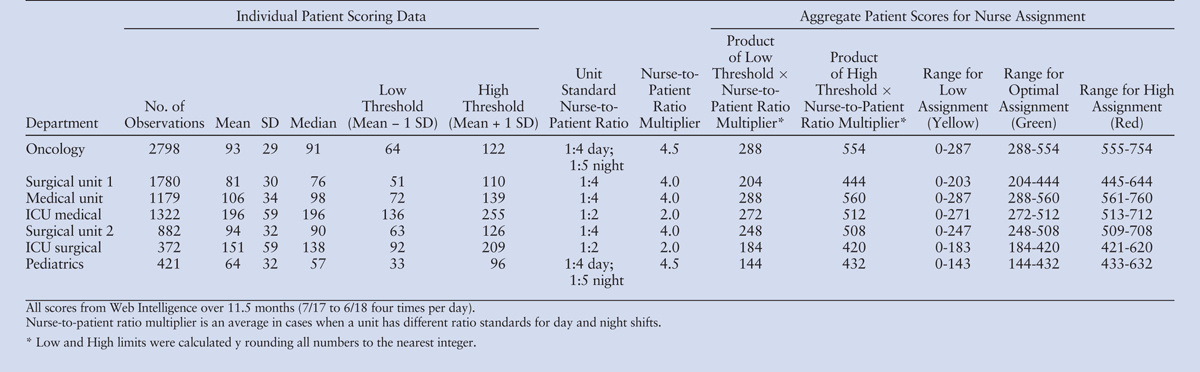
“The use of objective, electronically generated nursing workload scores, combined with traditional nurse-to-patient ratios, provides accurate real-time nurse staffing needs that can inform best practice in staffing.”
“Engagement with a course may improve academic performance, however, appropriate instruments are needed to measure engagement. Using an exploratory factor analysis approach, the 23-item Student Course Engagement Questionnaire (SCEQ) was used to quantify undergraduate nursing (n = 102), mid-wifery (n = 64), and paramedicine (n = 40) student engagement.” (Brown, et al)
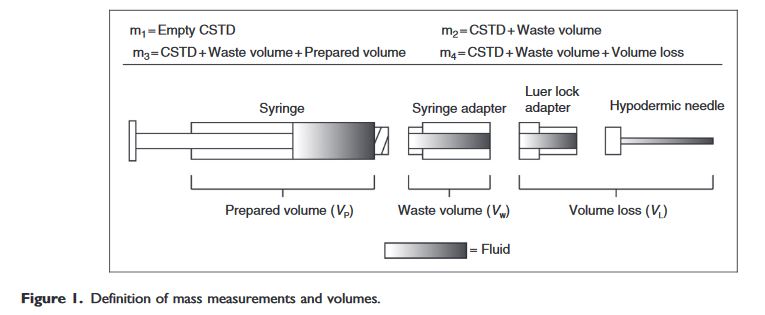
“While CSTDs are an important tool to reduce exposure to hazardous drugs, CSTD performance and design should be considered within the context of the varying tasks, users, and environments where they are used.”
“Today’s CNS scope of responsibilities encompasses micro, meso, and macro systems levels, and the impact is great. Role responsibilities vary widely, and positioning on the organization chart varies widely as well; CNSs are rising to the occasion. Although a strength of the CNS role can be the variability in the role responsibilities among healthcare settings, it has resulted in challenges in the delivery of education to best prepare for this vital advanced practice role.” (Coke)
“Nursing leaders responsible for orientation are challenged by the plethora of nursing knowledge and clinical skills required by nurses to provide safe care to critically ill patients. The goal is for new and experienced nurses to master the complexities of care and advanced technology and support the well-being of all. One way to achieve this goal is to actively engage new-to-practice nurses and experienced nurses in orientation programs designed to transfer knowledge and skills needed to provide bedside care”.(Monforto)
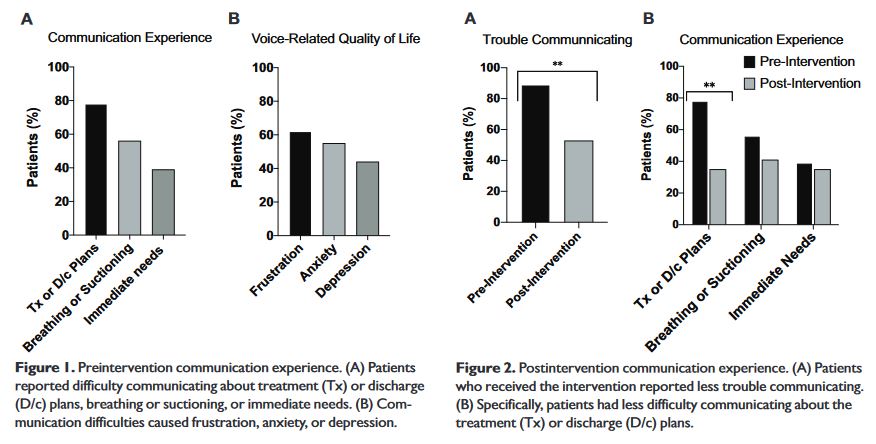
“Surgical procedures that render patients acutely aphonic can cause them to experience significant anxiety and distress. Participants in this study included hospitalized patients who acutely lost the ability to speak due to tracheostomy or total laryngectomy. Acute loss of phonation arising from surgery can be highly distressing for patients, and use of augmentative technology may alleviate some of these challenges by improving communication.”